Following the introduction of a surgical protocol that leveraged intraoperative imaging with a combination PET-CT scanner to assess the success of head and neck cancer resection, surgeons have used the technology for breast cancer.
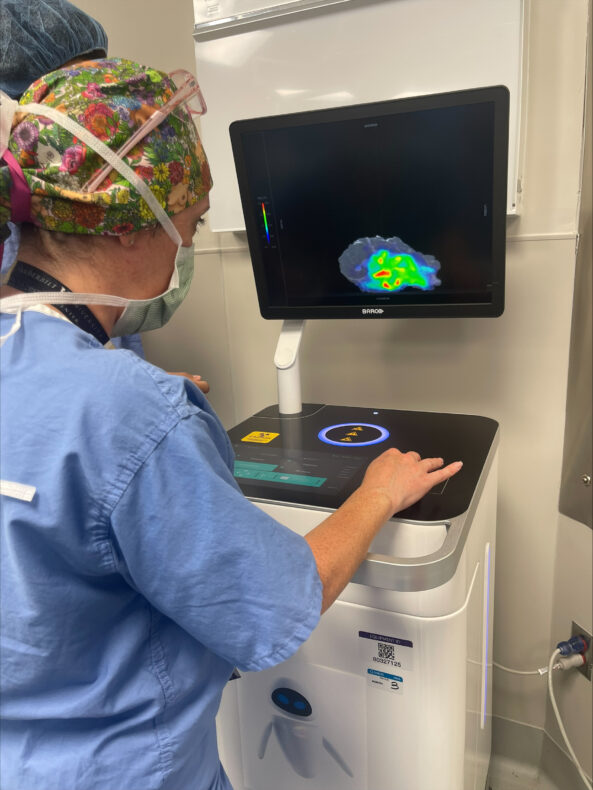
Denise Garcia, MD, uses the Xeos Aura 10 scanner to image a recently excised breast tumor from a patient. The use of the Xeos Aura 10 device ensures the imaging and assessment can be done in the operating room rather than in the pathology lab. (photo by Kyrionna Golliday)
Investigators led by Michael Topf, MD, Associate Professor of Otolaryngology-Head and Neck Surgery, performed the nation’s first surgery using intraoperative PET-CT scanning in September 2025. Now, a surgical team led by Denise Garcia, MD, Assistant Professor of Surgery in the Division of Surgical Oncology and Endocrine Surgery, has applied the technology to successfully resect a breast cancer mass.
“This application of intraoperative PET-CT is proof that countless patients can benefit from the expansion of this novel imaging methodology,” said Garcia. “Our team is proud to apply it to a type of tumor that has not yet been imaged for the purposes of assessing margin status. As our institution expands treatment methodologies to more types of cancer, we can cure more patients and give them peace of mind that their surgery has been completed with precision. This technological advancement underscores the success we’ve had across multiple disciplines in working toward that goal.”
Rapid expansion of intraoperative PET-CT scanning boosts efficiency, offers peace of mind to surgeons and patients alike
With each new application, surgeons are demonstrating that an intraoperative PET-CT imaging protocol can help reduce wait time for results from several days to a matter of minutes and allow surgical teams to know immediately whether they need to continue operating.
During surgery, the patient receives a dose of a radioactive agent that illuminates the cancer tissue in the scanner. Once the tumor is excised, it is placed in a specialized mobile PET-CT scanner called an Aura 10 device, developed and supplied by Belgium-based surgical technology company Xeos. The scanner negates the need to send the specimen to the pathology lab, providing surgical teams with a real-time view and allowing them to quickly determine if the entire cancerous mass was removed.
If any mass remains, the operation continues. If the cancer has been successfully resected, the surgery concludes, and the patient is sent home with peace of mind, knowing they won’t need to return for a follow-up surgery, and with confidence that their surgeons have a precise, immediate look at the results of the surgery. Because patients receive the radioactive agent on the day of surgery rather than in advance, they also receive a lower dose of radiation.
Allison Hanlon, MD, PhD, MBA (photo by Erin O. Smith)
As temperatures rise and more time is spent outdoors, dermatologists urge everyone to pay closer attention to their skin. According to the American Cancer Society, melanoma — the deadliest form of skin cancer — is expected to be diagnosed in more than 112,000 Americans this year as invasive disease, a figure that has climbed nearly 47% in the past decade. When caught early, melanoma is among the most treatable cancers, with a five-year survival rate around 99% for localized disease.
A vast majority of melanoma cases are linked to ultraviolet exposure from sunlight, making it largely preventable. Risk factors include fair skin, a history of sunburns (especially in childhood), numerous moles, and a family history of melanoma. But melanoma does not discriminate; it can develop in people of all skin tones and in areas that rarely see the sun.
Dermatologists recommend the ABCDE rule as a guide for self-examination:
Look for Asymmetry (one half of a mole doesn’t match the other),
irregular Borders,
uneven Color,
a Diameter larger than a pencil eraser, and
an Evolving shape, size or color.
Any spot that looks different from the moles around it — the so-called ugly duckling — also warrants professional evaluation. The most important step you can take is scheduling a routine skin check with a board-certified dermatologist.
“Early detection saves lives, and it starts with knowing your own skin,” says Allison Hanlon, MD, PhD, Professor and Chair of the Department of Dermatology at Vanderbilt Health. “When melanoma or another skin cancer is found early, our Mohs surgery team can often remove it completely in a single outpatient visit while preserving as much healthy tissue as possible.”
Mohs micrographic surgery is widely considered the gold standard for treating many skin cancers. Unlike standard excision, the Mohs technique examines 100% of the tissue margin under a microscope, layer by layer, until no cancer cells remain. The result is a cure rate of up to 99% for new skin cancers and the smallest possible wound, which is especially important for tumors on the face, ears, hands, and other cosmetically or functionally sensitive areas.
Vanderbilt Health’s Mohs Micrographic Surgery program brings together a fellowship-trained team of four Mohs surgeons: Hanlon; Anna Clayton, MD, Associate Professor of Dermatology and Director of the Micrographic Surgery and Dermatologic Oncology Fellowship; Stacy McMurray, MD, Assistant Professor of Dermatology and Associate Program Director for the Mohs Fellowship; and Emily Merkel, MD, Assistant Professor of Dermatology. The team collaborates with surgical and medical oncology specialists to develop individualized plans for even the most complex cases.
Mohs surgery at Vanderbilt Health is performed at Vanderbilt Dermatology, located at Vanderbilt Health One Hundred Oaks, 719 Thompson Lane in Nashville.
To schedule a skin cancer screening or learn more about Mohs surgery services, call 615-322-6485 or visit the Vanderbilt Health Dermatology website.
Eating, speaking clearly and breathing easily are essential functions we often take for granted, and Nick Schrock of Macon County, Tennessee, admits he did, too. Then, he noticed a small bump inside his mouth that changed everything.
He was just 30 when he felt a solid bump on the roof of his mouth where the hard and soft palates meet. It didn’t hurt and wasn’t irritated, so Schrock dismissed it as a random nodule of bone he just hadn’t noticed before. Nine months later, however, it began to grow and was soon the size of a quarter and felt “rubbery” rather than hard.
“It started to hurt when I yawned or took a bite of food,” he said. “It got bothersome, and I told my wife I needed to have it looked at.”
Today, after recovering from surgery at Vanderbilt University Hospital to remove what turned out to be a cancerous tumor and radiation therapy to target any remaining cancer cells, Schrock is grateful for all the care he’s received, but especially to have his voice back. Because of this, he feels he can be a better parent to his young daughter, Magnolia Mae, and can enjoy life with his wife, Brittany, and other family and friends.
After the tumor removal left a sizable hole inside his mouth, he initially could only speak in a muffled, lispy whisper. This was due to velopharyngeal insufficiency, a condition where the seal between the oral and nasal cavities does not close completely.
Schrock credits Vanderbilt University Medical Center providers for not only quickly addressing his cancer but also for restoring his voice. A key player on that collaborative team is Tyler Ames, DMD, chief of the Division of Dentistry at VUMC.
A custom obturator designed by VUMC’s Tyler Ames, DMD, sealed the hole left after removal of an oral cancer and restored Nick Schrock’s voice. It fits along the roof of the mouth, and the ball seals the cavity. (photo by Susan Urmy)
A rare cancer and arduous treatment
In January 2024, a biopsy revealed adenoid cystic carcinoma (ACC), a rare cancer typically originating in the salivary glands that makes up about 1% of all head and neck cancers. This type of cancer doesn’t run in families, and there are no known risk factors. While ACC is slow growing, it is aggressive. Surgery is the primary treatment, often followed by radiation. Reconstruction or prosthetics are often needed following treatment.
Because of the intricate anatomy of these areas of the body and often delayed detection, treatment for head and neck cancers can be arduous and impact critical functions like speaking, breathing and swallowing.
Within a week, the Schrocks were consulting with Alexander Langerman, MD, SM, a head and neck cancer and reconstructive surgeon at VUMC with fellowship training in microvascular reconstruction. Surgery was quickly scheduled.
Langerman worked for five hours to remove a golf-ball sized growth that was extensively invading the soft tissue and muscle, especially muscles involved with chewing. It required removal of part of Schrock’s upper jawbone and a few teeth. Langerman then performed a local flap surgery using part of Schrock’s inner cheek to help patch the hole inside his mouth.
Schrock then underwent radiation therapy under the care of D. Nathan Kim, MD, PhD, a Vanderbilt Health radiation oncologist at Vanderbilt-Ingram Cancer Center at Wilson County, which was much closer to his home.
Making it through 33 sessions of radiation treatment was one of the hardest things he’s ever done in his life, Schrock said. His mouth and throat were raw and dry. His stomach was continually upset. His hair, including his beard, fell out. And he lost 60 pounds.
And there were other setbacks. He lost hearing in his right ear because of a fluid buildup due to the radiation. That was resolved quickly through a minor procedure by otolaryngology-head and neck surgeon Matthew O’Malley, MD. Schrock also began having difficulty breathing through his nose. Another otolaryngology-head and neck surgeon, Naweed Chowdhury, MD, MPH, cleared swollen tissue caused by the radiation from a maxillary sinus, which improved his ability to breathe.
But the biggest thing he wanted resolved was his voice. Ames was ready. He had been in consultation with Langerman from the start of Schrock’s journey, viewing imaging and following his progress closely.
“Nick expressed that he was afraid of his daughter being embarrassed by his speech,” Ames said. “I took this to heart as I also have a young daughter. Putting myself in his shoes, I knew that I had to do everything I could to help him.
“With these cases you really are not sure what is possible until you try. Nick is an amazing patient who is very motivated. His drive helped to keep the treatment on track and helped motivate me to do the best I could for him.”
Prosthetics to seal oral cavity holes
When individuals are left with holes or deficits in their oral cavity due to congenital defects like cleft palate, cancer surgeries or trauma, prosthetics known as obturators are often custom designed to restore function. This is what Schrock needed.
“An obturator is a prosthetic device used to close and seal a defect or opening in the hard or soft palate to assist in speech and eating and drinking,” Ames said. “This can prove challenging because you are not always sure if the patient is going to tolerate having the obturator in the back of their throat.”
Because of the precision diagnoses and effective treatments provided by Vanderbilt-Ingram clinicians, patients come not just from Tennessee but also from parts of seven contiguous states and beyond. That means the center sees a higher volume and higher complexity of patients with head and neck cancers. Ames was increasingly being referred individuals who needed restoration after surgery.
Obturators are usually created by specialized dentists known as prosthodontists or maxillofacial prosthodontists, but many private practices instead focus on dental implants and other higher volume, profitable procedures. Finding a dentist who can create a custom obturator isn’t easy. With the growing number of cancer patients he was seeing with unique needs, Ames decided a few years ago he would research and teach himself the precision craft of creating obturators.
“Since Tyler joined VUMC, we have worked together in tougher and tougher cases and grown together as partners,” Langerman said. “Nick’s case was indeed a tough one, and his success is the product of the years of work Tyler has put in to restore patients to a greater quality of life after surgeries such as this.”
Ames works with Vanderbilt Health surgical oncologists to review imaging, even running over to the surgical clinics so he can see the space he needs to seal. He works with an area dental lab to produce obturator prototypes and in the early days, he even tried varied materials to achieve the best seals and most comfortable devices. Now, though every case is different, he has become adept at problem-solving and creating obturators for even highly complex cases.
“In Nick’s case, a nasal endoscopy performed by Dr. Langerman with the custom obturator in allowed me to have a ‘GPS’ to show exactly where I needed to add to the obturator to better seal the defect and aid his speech,” Ames said. “We could see the obturator in place from the viewpoint of the sinus, which helped tremendously.”
Recently, Ames met with Schrock again and checked in on his progress. His voice was strong and easily understandable. But Ames cocked his head, listened closely, and told Schrock he felt like he could make some minor adjustments to improve his voice even more. Schrock smiled.
“Dr. Ames has significantly changed my life,” Schrock said. “I still struggle, and I don’t like talking in front of a lot of people, but what he’s done for me is incredible.
“I don’t mind sharing my story if it gives someone else hope. It does get better. I didn’t feel that way for a while, but it does.”
Mark Kelley, MD, MMHC, medical director of the Williamson County General Surgery Division in the Department of Surgery at Vanderbilt University Medical Center, has retired, effective Oct. 1, after 28 years of exceptional service and leadership.
“Dr. Kelley transformed the Division of Surgical Oncology and Endocrine Surgery into one of the nation’s largest and most productive academic surgical oncology programs,” said Carmen Solórzano, MD, John L. Sawyers Chair in Surgical Sciences and chair of the Department of Surgery. “His remarkable contributions span clinical excellence, innovative research and impactful education.”
Kelley, an associate professor of Surgery in the Division of Surgical Oncology and Endocrine Surgery, is lauded by his colleagues and surgical leaders for his contributions both at VUMC and nationally.
“Dr. Kelley’s career reflects an unwavering commitment to excellence in clinical care, research, education and leadership,” said Seth Karp, MD, H. William Scott Jr. Chair in Surgery and chair of the Section of Surgical Sciences. “His legacy has profoundly shaped surgical oncology at Vanderbilt and beyond. We are grateful for his dedication and leadership.”
In 1997, Kelley joined the VUMC faculty as an assistant professor in the newly established Division of Surgical Oncology and Endocrine Surgery and served as clinical director of the Vanderbilt Breast Center until 2005. His leadership skills led to his appointment as chief of the Division of Surgical Oncology and Endocrine Surgery in 2002, a role he held until 2015.
“As clinical director of the Vanderbilt Breast Center, he led its development and transition from a small practice in the Village at Vanderbilt to a comprehensive breast center at One Hundred Oaks,” said Solórzano. “In 2005, he passed the clinical directorship to Dr. Ingrid Meszoely, whom he recruited back to Vanderbilt after her surgical oncology fellowship. Today, the Vanderbilt Breast Center is one of the largest and most comprehensive programs in the United States.”
Recognizing the importance of focused training in breast surgical oncology, Kelley developed the framework for a breast surgical oncology fellowship. Expansion of the curriculum under the leadership of Mary Hooks, MD, MBA, and Ingrid Meszoely, MD, led to accreditation of the program by the Society of Surgical Oncology in 2016.
Under Kelley’s leadership, the Division of Surgical Oncology and Endocrine Surgery expanded from four surgeons to a multidisciplinary team of more than 20 surgeons, advanced practice providers (APPs) and research scientists. He also played a pivotal role in recruiting and mentoring key faculty who now serve as VUMC surgical and Vanderbilt-Ingram Cancer Center leaders, including Rondi Kauffmann, MD, MPH; Christina Bailey, MD, MSCI; Kamran Idrees, MD, MSCI, MMHC; Meszoely, Solórzano and others.
Kelley was a sought-after mentor throughout his career, and assisted numerous medical students, surgical trainees and junior faculty as they participated in projects and developed their own research. Under his leadership, the Division of Surgical Oncology and Endocrine Surgery was highly ranked, year after year, as a favorite learning environment for general surgery trainees. More than 30 residents completed surgical oncology fellowships during Kelley’s tenure, and many are leaders in the field today, including five current VUMC faculty members.
He was an early advocate for the integration of APPs into clinical roles. In 1999, he established training and mentorship programs for APPs specializing in breast health and surgical oncology, and these programs served as models for integrating APPs into surgical practices throughout VUMC. Today, there are 10 APPs practicing in inpatient and outpatient roles in the Division of Surgical Oncology and Endocrine Surgery.
Kelley was a surgical innovator and the first surgeon in Tennessee to perform sentinel lymph node biopsy for breast cancer and melanoma in 1997. This procedure has transformed the care of these cancers. Kelley developed an Institutional Review Board (IRB)-approved protocol to train surgeons on this technique, leading to the rapid and safe application of the new surgical procedure at VUMC and in the community.
Kelly was also integrally involved in the development of multidisciplinary clinical and research programs at Vanderbilt-Ingram Cancer Center. From 2000-2012, he served as chair of the VUMC Cancer Committee. This group monitors and reports cancer volumes and outcomes, guides quality improvement, and ensures compliance with national cancer treatment standards. During his tenure as chair, VICC was continuously accredited by the American College of Surgeons Commission on Cancer. The program was also routinely recognized as one of the top National Cancer Institute-accredited comprehensive cancer centers nationwide during that time.
Early in his career, Kelley had an independent laboratory that focused on translational research in melanoma tumor biology and contributed to the early development of immunotherapy for melanoma. He established the melanoma and cutaneous malignancy tissue repository in 2003. This IRB-approved research repository has collected tumor tissue samples from patients undergoing surgical resection or biopsy with paired clinical data from more than two decades. This invaluable resource has supported high impact basic and translational studies that have led to novel combinations of immunotherapy and targeted therapy being investigated in clinical trials today.
“Dr. Kelley is highly committed to the advancement of cancer care through research, and we are grateful that he will remain active in clinical and translational research with VUMC and VICC as professor of Surgery, retired, to continue to improve care for patients with cancer,” said Karp.
In a collaboration between Vanderbilt University Medical Center’s Department of Otolaryngology-Head and Neck Surgery and the Vanderbilt University School of Engineering, investigators have received a $2.5 million grant to develop a head-mounted augmented reality system that can guide surgeons in ensuring complete tumor removal in head and neck cancer surgery and potentially reduce the recurrence rate of tumors.
The National Institutes of Health grant was awarded to primary investigator Jie Ying Wu, PhD, assistant professor of Computer Science, with secondary appointments in Biomedical Engineering, Electrical and Computer Engineering, and Mechanical Engineering at Vanderbilt University. Wu also has an appointment in the Department of Surgery at Vanderbilt University Medical Center.
Co-investigators include Michael Miga, PhD, director of the Vanderbilt Institute for Surgery and Engineering and the Harvie Branscomb Professor and chair of the Department of Biomedical Engineering, as well as Michael Topf, MD, associate professor of Otolaryngology-Head and Neck Surgery, and Matthew Weinger, MD, professor of Anesthesiology and Biomedical Informatics.
“I am delighted to receive this award to transform surgical care for head and neck cancer,” said Wu. “This funding will allow us to build novel deformation models for heterogeneous tissue shrinkage and ensure the augmented reality software design is intuitive for surgeons and fits within the clinical workflow.”
The development of the technology stems from a deficit Topf noticed in surgical oncology. While three-dimensional scanning has become part of the norm for other aspects of patient care, from same-day dental crowns to prosthetic limbs, Topf was troubled by the lack of application for 3D scanning in oncologic surgery. Topf implemented a protocol to create 3D models of resected cancers for surgeons, pathologists and oncologists to reference.
“We came up with a way to 3D scan a surgical specimen in real time in less than 10 minutes prior to processing and not interfere with all the other important things that are going on in the pathology lab,” said Topf. “Encouragingly, this is a widely transferable practice and would be applicable to most cancer surgeries, from orthopaedic oncology to breast cancer.”
Weinger, who is a faculty member of the Center for Research and Innovation in Systems Safety (CRISS) at VUMC, expressed the organization’s eagerness to support the research.
“CRISS is excited to contribute to this important project, applying advanced engineering to ensure the user interface of this technology guides surgeons to safely and effectively treat cancer patients,” said Weinger, who holds the Norman Ty Smith Chair in Patient Safety and Medical Simulation.
Safety and effectiveness are at the core of the research. As Miga explained, the 3D mapping technology will allow surgeons to rely less on a fallible mental construction of the resection plane, thereby reducing the risk of human error affecting the procedure.
“When it comes to cancer surgery, surgeons often say, ‘We think we got it all,’” said Miga. “What many don’t realize is that every operation requires the surgeon to construct a mental spatial map, linking the visible surgical field to their internal understanding of the tumor’s extent. It’s an incredibly complex task, and sometimes, despite best efforts, reoperations are necessary.
“Now imagine if, while the patient is still on the table, we could detect the margin in real time, and then, using a holographic overlay, highlight the precise region that needs further attention. Through our collaboration, that’s the kind of transformation we’re seeking to make commonplace with this research.”
Collaboration has been consistent over the last few years between the Medical Center and the University, said Wu. She hopes research into the technology will eventually support a clinical trial, a sentiment shared by Eben Rosenthal, MD, Barry and Amy Baker Professor and chair of the Department of Otolaryngology-Head and Neck Surgery.
“Improving surgical outcomes is of the utmost importance, especially when it comes to ensuring total tumor removal and reduced risk of recurrence for cancer patients,” said Rosenthal. “The research supported by this grant will help us perfect this technology as we seek practical applications for patient care, including clinical trials and, eventually, everyday use in the operating room.”
A study published in the journal JAMA Surgery demonstrated the benefits of using fluorescence-guided imaging to assess margins in head and neck cancer. Researchers at Vanderbilt University Medical Center found that leveraging data collected both during surgery (in vivo) and after the tumor’s removal (ex vivo) can help guide surgeons in achieving a negative margin in cancer resection.
A margin refers to the areas around the tumor being removed. The desirable outcome is to complete surgery with a negative margin, indicating that no cancer was found at the edge of the resection. A positive margin indicates that cancer cells remain in the tissue, which increases the risk of recurrence and reduces the chance of survival.
To assess those margins, surgeons may use fluorescent agents administered to the patient’s tissue. Systemically infused agents have been shown to differentiate cancerous and healthy tissue with high accuracy.
“Our research found that the use of fluorescence imaging both internally and externally can improve surgeons’ ability to precisely and safely excise tumors,” said Shravan Gowrishankar, MD, a research fellow in the Department of Otolaryngology-Head and Neck Surgery and the study’s first author. “This research seeks to illuminate methods of leveraging fluorescence imaging to achieve negative margins, particularly for deep resections, which often prove difficult.”
This figure illustrates an example of a tumor with two types of margins: mucosal, which surrounds the surface of the tumor, and deep, which is healthy tissue beyond the tumor. Deep margins are more difficult to navigate for surgeons, but fluorescence imaging seeks to change that. (courtesy of researchers)
The researchers defined two classifications of margins: the superficial or mucosal margin refers to the area uninvolved with the tumor but surrounding its surface, while the deep margin refers to the 4 to 5 millimeters of healthy tissue beyond the tumor’s most invasive points, or the depth of normal tissue between the tumor edge and the cut surface of the specimen.
“Currently, it’s easier to achieve negative mucosal margins than deep margins,” said corresponding author Eben Rosenthal, MD, chair of the Department of Otolaryngology-Head and Neck Surgery and Barry and Amy Baker Professor of Laryngeal, Head and Neck Research. “Deep margins aren’t able to be assessed as easily because surgeons must rely on estimation of the distance from the tumor to guide the resection.
“We sought to improve methods of achieving negative margins across the board because estimation isn’t good enough where patient safety is concerned.”
The assessment of deeper margins is further confounded during surgery by tissue retraction and the presence of blood, which can obscure the view of the surgeon. And while autofluorescence — a process by which naturally occurring chemicals in the tissue can absorb light of a particular wavelength and reemit it at a different wavelength — can help surgeons assess mucosal margins, deeper margins are impossible to assess via this process because the light does not penetrate beyond a millimeter.
To assist in ensuring a negative margin in a deep resection, surgeons can use fluorescence imaging techniques. Mapping tumors after resection can provide data on how close the margins are to the surface of the deep resection, and intraoperative in vivo fluorescence imaging can reveal areas of residual disease in the tumor bed. In combination, the information provided by both methods of fluorescence imaging can guide further examination and sampling to help achieve fuller resection of the deep margin.
While both methods in combination are critical to achieving better outcomes in surgery, said Gowrishankar, ex vivoimaging devices have certain advantages over in vivo hardware.
Shravan Gowrishankar, MD
“While the data we get from in vivo imaging is valuable, it’s largely qualitative because of variance in ambient light in the operating room,” said Gowrishankar. “Ex vivo imaging is more precise because we can seal out external light in a controlled environment to measure fluorescence intensity and guide our assessment of deep margins.”
In ex vivo imaging, fluorescence intensity increases the closer the tumor tissue approaches the cut surface of the tumor specimen, and data from this measurement can be used to create a sort of “heat map” measuring the relative depth of the tumor across the entire specimen. By using this imaging technique, surgeons can more precisely detect the reach of cancer cells in the tissue and perform precise resections.
“Mucosal margins are easy enough to detect during surgery without fluorescent agents, but those agents are critical in helping us close the gap with deep margins,” said Rosenthal. “Missed deep margins contribute to the majority of positive margins after resection, which in turn contribute to negative health outcomes for patients. Large-scale adoption of these techniques will have a meaningful impact on the health of patients who undergo surgery to remove cancerous tumors.”
Additional authors from Vanderbilt University Medical Center include:
Jennifer Choe, MD, PhD, assistant professor of Medicine in the Division of Hematology Oncology
Alexander Langerman, MD, SM, FACS, associate professor of Otolaryngology-Head and Neck Surgery
Kyle Mannion, MD, FACS, associate professor of Otolaryngology-Head and Neck Surgery
Aviva S. Mattingly, MD, MS, VTOPS/R25 Research Resident
Sarah L. Rohde, MD, MMHC, associate professor of Otolaryngology-Head and Neck Surgery and division director of Head and Neck Oncologic Surgery
Robert Sinard, MD, FACS, professor of Otolaryngology-Head and Neck Surgery
Hidenori Tanaka, MD, PhD, visiting assistant professor of Otolaryngology-Head and Neck Surgery
Michael Topf, MD, MSCI, assistant professor of Otolaryngology-Head and Neck Surgery.
This research was supported by the National Cancer Institute, part of the National Institutes of Health (grants R01CA279249, R01CA239257, R01CA266233 and R01CA238686).
Aimal Khan, MD, assistant professor of Surgery at Vanderbilt University Medical Center, noticed the puzzled or anxious expressions of patients trying to fully comprehend what he was saying during preoperative consultations, so he devised visual aids — three-dimensional models of the lower digestive tract.
The 3D models allowed patients to easily distinguish the ascending colon from the sigmoid colon, along with other parts of the digestive system. Patients could actually see where the surgery would occur, and Khan noticed that they asked more questions, felt more confident and seemed less anxious. He devised a study to determine whether his personal observations were scientifically valid.
The study, which was published June 3 in JAMA Network Open, determined that the 3D models made patients feel they played a bigger role in decision-making and that their anxiety levels decreased.
The patients were scheduled for partial or complete colon and/or rectal resections for colorectal cancer, diverticulitis or inflammatory disease. Fifty-one patients participated in the study with 28 receiving consultations using the 3D models and 23 receiving conventional consultations. The patients in the 3D arm of the study reported a significantly higher involvement in shared decision-making and significantly reduced anxiety levels compared to the other patients.
Khan and five other Vanderbilt surgeons conducted the study from March 2022 to June 2023.
“Using 3D models during consultations allowed our patients to truly visualize their surgery, which not only empowered them to take an active role in decision-making but also significantly eased their anxiety. This approach has the potential to transform how we communicate complex information to our patients. We are currently working with surgeons from other specialties, including thoracic surgery, ENT and surgical oncology, to validate these findings in a multicenter randomized trial,” Khan said.
The findings are important because other studies have shown that improvements in shared decision-making are associated with reduced hospital stays, lower health care utilization, improvement in patient-reported health outcomes and fewer emergency department visits.
The 3D models used in the study were developed in collaboration with the Department of Radiology. The modular designs, which were made with 3D printing, allowed each segment of the colon and rectum to be magnetically detached and reattached.
To the knowledge of the study’s authors, this is the first randomized clinical trial to compare the effectiveness of a 3D-printed model with usual care on colorectal surgery patients’ involvement in decision-making, anxiety and education.
Other Vanderbilt researchers who authored the study are Danish Ali, MD, Shannon McChesney, MD, Michael Hopkins, MD, Molly Ford, MD, Roberta Muldoon, MD, Timothy Geiger, MD, MMHC, Alexander Hawkins, MD, MPH, Georgina Sellyn, MA, Hillary Samaras, RN, and Dann Martin, MD, MS.